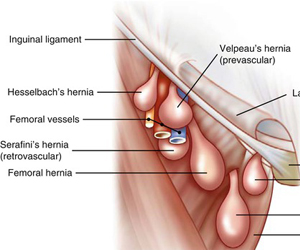
 These are the hernias seen in the groin arising in the inguinal or femoral canal. The origin of these hernias is either deep inguinal or femoral orifices which are natural orifices allowing exit of normal vascular structures like blood vessels to testes or legs. When these openings are weakened or widened either at birth or by muscle weakness, the abdominal structures protrude through them and form hernias. These are hence more commonly seen in men though some women also can be affected. They can occur in children when the defect remains abnormally open or in adults when the defect stretches due to weakened abdominal muscles.
These are the hernias seen in the groin arising in the inguinal or femoral canal. The origin of these hernias is either deep inguinal or femoral orifices which are natural orifices allowing exit of normal vascular structures like blood vessels to testes or legs. When these openings are weakened or widened either at birth or by muscle weakness, the abdominal structures protrude through them and form hernias. These are hence more commonly seen in men though some women also can be affected. They can occur in children when the defect remains abnormally open or in adults when the defect stretches due to weakened abdominal muscles.
Initially people either notice pain in the groin or around the umbilicus on exertion. Majority of people notice a swelling in their groin which increases on standing or exertion. When these are neglected the hernia follows the following course
- Gradual enlargement: The hernia increases in size gradually and descend into the scrotum. In later stages the hernia doesn’t subside on lying down which is called as irreducible hernia.
- Obstruction/ Strangulation: Sudden blockage of intestinal contents because of a twist of the intestine when it is called as obstructed hernia. This causes severe pain, vomiting, abdominal bloating and inability to pass wind/ stools. This needs emergency surgery, else the intestinal contents may get devitalized when it is called as strangulated hernia which can be fatal.
Because of the narrow openings and the oblique course of the contents, these are more prone for complications.
All hernias need a surgical correction whenever patient is fit enough for surgery. When diagnosed early, surgery can be performed laparoscopically for painless and fast recovery. Patients presenting with large hernias or complicated irreducible/ obstructed hernias need an emergency open operation.
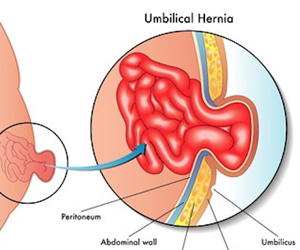 A hernia is defined as an abnormal protrusion of an organ through a defect in the cavity containing the organ. Abdominal hernias occur when visceral organs protrude through a muscle defect. These may be natural defects like umbilicus (umbilical hernia), inguinal ring (inguinal/ groin hernia) or through postoperative scar (incisional/ ventral hernia).
A hernia is defined as an abnormal protrusion of an organ through a defect in the cavity containing the organ. Abdominal hernias occur when visceral organs protrude through a muscle defect. These may be natural defects like umbilicus (umbilical hernia), inguinal ring (inguinal/ groin hernia) or through postoperative scar (incisional/ ventral hernia).
Incisional hernias are the hernias which occur at the site of a previous surgical scar and are increasingly becoming common. These occur due to weakening of the scar which can be because of
Wound infection: Infections in the early postoperative period impair healing and cause a weak scar.
Inadequate postoperative support: Early resumption of strenuous activity after surgery like lifting weights puts excessive strain on the scar before it has regained strength.
Pregnancy related: Women tend to have a higher risk of hernia after caesarian section since the muscles already stretched because of pregnancy.
All hernias have a propensity to lead to complications if left untreated. Complications occur when the contents of the hernia get kinked or compressed in the hernia leading to intestinal obstruction initially and strangulation later. Complicated hernias can be life threatening and need an emergency surgery. Treatment is exclusively a surgical repair using a prosthetic mesh whenever feasible. The key principles of surgery include safe restoration of contents to their original location followed by a tension free repair with an adequately sized mesh. Previously smaller hernias used to be repaired laparoscopically while large or complicated ones needed open repair. Nowadays advances in laparoscopy like eTEP ensure even large hernias can be treated laparoscopically.
 Recurrence is a complication known to happen after a hernia repair and is a major concern for patients. Treatment of recurrent hernia needs to be individualised to the patient depending on the medical conditions of the patient, details of the previous surgery and the nature of the recurrence. However, recent advances in laparoscopic and robotic surgeries widen the options for treatment and improve the results. Identification and treatment of the causative factors like cough and constipation is essential prior to planning the surgery. Proper defect closure, adequate size of mesh and tension free repair are the key principles involved in optimal outcome. Newer techniques like eTEP, component separation and hybrid repair ensure lesser postoperative pain and recurrence.
Recurrence is a complication known to happen after a hernia repair and is a major concern for patients. Treatment of recurrent hernia needs to be individualised to the patient depending on the medical conditions of the patient, details of the previous surgery and the nature of the recurrence. However, recent advances in laparoscopic and robotic surgeries widen the options for treatment and improve the results. Identification and treatment of the causative factors like cough and constipation is essential prior to planning the surgery. Proper defect closure, adequate size of mesh and tension free repair are the key principles involved in optimal outcome. Newer techniques like eTEP, component separation and hybrid repair ensure lesser postoperative pain and recurrence.