 Liver tumors are increasingly becoming common and is the fifth most common cause of cancer related deaths. Theses can broadly be divided into the following groups
Liver tumors are increasingly becoming common and is the fifth most common cause of cancer related deaths. Theses can broadly be divided into the following groups
- Primary Hepatocellular Cancer (HCC): These tumors originate from the liver cells. Primary liver tumors are increasingly common because of the prevalence of cirrhosis (secondary to alcohol or non-alcoholic fatty liver disease) and viral hepatitis (B and C). Other risk factors include some inherited diseases like hemosiderosis and exposure to carcinogens.
- Cholangiocarcinoma: These tumors originate from the bile ducts and behave differently from the primary HCCs. They are more common in patients with biliary diseases like sclerosing cholangitis and choledochal cysts.
- Metastatic tumors: secondary tumors from the other organs spread to the liver. Here treatment is dependent on the site of origin of the tumors. Since these are already advanced, outcomes are poor in this subset of patients.
Since liver is a large organ and has good functional reserve, symptoms like pain and jaundice appear relatively late. majority of patients initially present with non specific symptoms like weight loss, lack of appetite and fever. High degree of clinical suspicion and screening is needed for early diagnosis of these tumors. Diagnosis can be established with CECT or MRI of the abdomen. Unlike other tumors biopsy is not essential in all patients since it can lead to complications like bleeding and tumor spread.
Treatment is dependent not only on the stage of the tumour but also the functional capacity of the native liver and performance status of the patients. Surgical resection is offered to patients with early tumours in an otherwise normal liver. Transplant is an option in patients who have early tumours in the background of cirrhosis. Patients with advanced tumours or with poor general condition can benefit from interventional radiology(TACE/TARE) or chemotherapy (targeted therapy like sorafenib). Tumours from the biliary tract are called cholangiocarcinoma and present with pain or jaundice. These are relatively slow growing tumours and benefit from surgical resection if diagnosed early.
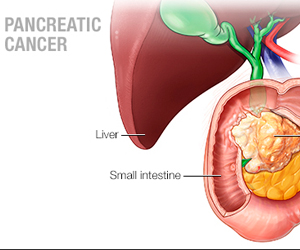 Pancreas being a deep seated organ results in delayed onset of symptoms thus making screening essential for early diagnosis. Pancreatic tumors present problems in treatment due to their deep location and relation to important blood vessels. Grossly pancreatic tumors are of three types
Pancreas being a deep seated organ results in delayed onset of symptoms thus making screening essential for early diagnosis. Pancreatic tumors present problems in treatment due to their deep location and relation to important blood vessels. Grossly pancreatic tumors are of three types
- Ductal tumors: Majority of tumors arising in pancreas originate from the ductal tissue (ductal adenocarcinoma). These are very aggressive tumors and early diagnosis is important for a good outcome.
- Cystic tumors: These are more commonly seen in younger patients. They usually grow rapidly and present as large tumors. However since they tend to remain localized to pancreas, surgery offers lasting cure in these patients.
- Rare tumors: Tumors like IPMN are rare but now being increasingly detected on screening.
Pancreas being a deep seated organ results in delayed onset of symptoms thus making screening essential for early diagnosis. The common risk factors include smoking, obesity, hereditary (BRCA 2 mutations) and chronic pancreatitis. Patients usually complain of pain radiating to back, jaundice, vomiting and unexplained weight loss. Worsening of diabetes in chronic pancreatitis is also an early sign.
Diagnosis is usually established after a contrast enhanced CT scan or ERCP. Treatment and outcome exclusively depend on the stage of the tumor. Patients with early tumors benefit with pancreatectomy followed by chemotherapy. Patients with advanced tumors usually are very sick and only palliative care is offered.
 Cancers involving esophagus or food pipe are increasingly common in older age groups. The main types of tumors involving esophagus include
Cancers involving esophagus or food pipe are increasingly common in older age groups. The main types of tumors involving esophagus include
- Squamous cell cancers: These are the most common tumors and involve upper and middle segments of the esophagus.
- Adenocarcinoma: These involve lower segment of the esophagus adjoining the stomach. These are more prone in patients with GERD. These resemble gastric cancers in clinical behavior and symptoms and hence their treatment is also different from squamous cell tumors.
- Rare tumors: Leiomyoma, GIST and leiomyosarcoma are rare tumors and treatment is individualized.
The main risk factors for these tumors are smoking and long standing reflux disease. Patients usually present with difficulty in swallowing (dysphagia), hoarseness of voice and weight loss. Patients giving history of difficulty in swallowing need to undergo upper GI endoscopy for evaluation. Diagnosis is established after upper GI endoscopy and biopsy of the tumor. PET scan is needed for assessing the extent of the tumor and assessing curability.
Treatment options depend on the extent of the disease and location of the tumors. Patients with advanced tumors are treated with chemotherapy and radiation. Stereotactic radiotherapy and endoluminal stents help in symptomatic relief inpatients with advanced cancers. Cancers of the upper esophagus are primarily treated with radiation and chemotherapy. Tumors of the middle and lower thirds need multimodality treatments. Surgery in addition to chemoradiation is the main stay of treatment. Surgery involves radical esophagectomy. This can now a days be performed with minimal access thoracoscopy for faster recovery.
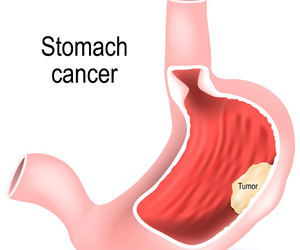 Gastric cancer is the third most common cause for cancer related deaths. There are three types of tumors affecting stomach which include
Gastric cancer is the third most common cause for cancer related deaths. There are three types of tumors affecting stomach which include
- Gastrointestinal stromal tumors (GIST): These originate from the all of stomach and usually present as large lumps. Despite their size, they have relatively good outcomes. Majority do not spread beyond stomach. Even for patients who have advanced tumors, targeted therapy in the form of Imatinib improves outcomes.
- Gastric Lymphomas: These arise from the lymphoid cells within the stomach. Chemotherapy is the main line of treatment. Surgery is rarely required. Due to recent advances in chemotherapy, outcomes have improved.
- Gastric adenocarcinoma: Majority of gastric cancers are adenocarcinomas which are highly aggressive.
Early symptoms include symptoms of acidity worsening despite medicines, especially in older patients. With advancing disease, patients complain of pain and vomiting, occasionally blood stained. Sometimes patients may present with non specific complaints like weight loss and loss of appetite, and in these patients diagnosis is possible only after endoscopy.
Major risk factors for gastric cancers include
Helicobacter pylori infection: H pylori is the most common cause for gastritis and duodenal ulcer and is very common in South India. Patients who have long standing H pylori gastritis have a higher risk of gastric cancer. Hence tseting for H pylori and eradication treatment is highly recommended in patients with symptomatic gastritis.
Genetic: Patients with a strong family history of gastric cancer have approximately double the risk and screening with endoscopy is advised in patients over 50 years of age.
Environmental: Smoking, obesity and food additives are proven to increase the risk of gastric cancer. Since these are reversible, it is advisable to correct life style accordingly.
Any patient above middle age presenting with acidity, those with progressive symptoms despite medications or blood stained vomiting needs to be evaluated with an upper GI endoscopy to screen for gastric cancers. This is all the more important since stage of the tumor at the time of diagnosis is the single most important factor in determining the overall outcome of treatment in these patients. CECT or PET scan is needed for assessing the extent of tumors. Surgery in the form of radical gastrectomy followed by chemotherapy is the standard treatment for early stage gastric cancers. For patients with advanced tumors, treatment is usually chemotherapy and palliative gastrojejunostomy or antral stenting for relief of vomoiting.